Per the American Physical Therapy Association’s (APTA) “Defensible Documentation Tips” resource¹, the top 10 payer complaints about documentation (reasons for denials) include:
1. Poor legibility
2. Incomplete documentation
3. No documentation for date of service
4. Abbreviations – too many, cannot understand
5. Documentation does not support billing (coding)
6. Does not demonstrate skilled care
7. Does not support medical necessity
8. Does not demonstrate progress
9. Repetitious daily notes showing no change in patient status
10. Interventions with no clarification of time, frequency, duration
Many of these items can be addressed with strong documentation that conveys underlying impairments, objective tests & measures, technical preparation and parameter selection, skilled intervention provided by the therapist to the patient/client before, during, and after a mode of treatment, and the patient performance and progress. Below are examples of how these documentation principles can be implemented:
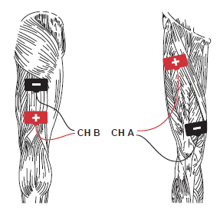 PENS – Transfer training and patterned NMES, LE triphasic (knee flexion/extension protocol) 3x/week x 15 minutes to the bilateral LEs for neuromuscular re-education to improve sit to stand transfer ability. 2x4 reusable electrodes used with intensity around 65mA for each channel until a visible twitch observed. Intensity regularly adjusted during treatment to maintain a light twitch. Patient given verbal and tactile prompts during treatment to perform repeated knee extension exercise. Skin prepped and assessed prior to and after treatments. Patient reports increased ease getting in and out of the car and now able to perform 5 sit to stand reps in 30-seconds vs. 1 rep one week ago.
PENS – Transfer training and patterned NMES, LE triphasic (knee flexion/extension protocol) 3x/week x 15 minutes to the bilateral LEs for neuromuscular re-education to improve sit to stand transfer ability. 2x4 reusable electrodes used with intensity around 65mA for each channel until a visible twitch observed. Intensity regularly adjusted during treatment to maintain a light twitch. Patient given verbal and tactile prompts during treatment to perform repeated knee extension exercise. Skin prepped and assessed prior to and after treatments. Patient reports increased ease getting in and out of the car and now able to perform 5 sit to stand reps in 30-seconds vs. 1 rep one week ago.

ULTRASOUND – Subthermal ultrasound followed by manual therapy 5x/week to right knee contusion to increase local circulation and decrease pain prior to ambulation. US 3MHz, 20% duty cycle, 0.5W/cm² x 5 min. Patient’s pain decreased to 4/10 from 8/10 and now ambulates 25 feet vs. 5 feet one week ago.
 DIATHERMY – SWD at 4 delta T x 20 min with towel to the right elbow to increase tissue temperature and extensibility prior to manual therapy and stretching. Orthotic set to -35 degrees and applied after manual therapy to reduce right elbow flexion contracture to improve ability to dress and feed self. During SWD treatment patient regularly repositioned for optimal treatment alignment and to maintain prolonged stretch. Patient able to actively move through available range (measured with a goniometer) of 36° - 100° this week vs. 44° - 100° one week ago.
DIATHERMY – SWD at 4 delta T x 20 min with towel to the right elbow to increase tissue temperature and extensibility prior to manual therapy and stretching. Orthotic set to -35 degrees and applied after manual therapy to reduce right elbow flexion contracture to improve ability to dress and feed self. During SWD treatment patient regularly repositioned for optimal treatment alignment and to maintain prolonged stretch. Patient able to actively move through available range (measured with a goniometer) of 36° - 100° this week vs. 44° - 100° one week ago.
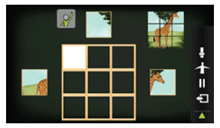 OMNIVR® – Bilateral UE therapeutic exercise via virtual reality system puzzle exercise at mod level reach to improve lateral and overhead reach for improved ability to dress independently. Therapist provided min tactile and verbal assistance to complete last 25% of desired range. Mod assistance required through greater than 50% of range one week ago and improvement in FIM self-care upper body dressing noted from 3 (mod assist) to 4 (min assist).
OMNIVR® – Bilateral UE therapeutic exercise via virtual reality system puzzle exercise at mod level reach to improve lateral and overhead reach for improved ability to dress independently. Therapist provided min tactile and verbal assistance to complete last 25% of desired range. Mod assistance required through greater than 50% of range one week ago and improvement in FIM self-care upper body dressing noted from 3 (mod assist) to 4 (min assist).
References:
1. www.apta.org/DefensibleDocumentation