Speech-language pathologists (SLPs) are commonly involved in the rehabilitation of patients with cardiopulmonary disorders. Patients hospitalized with respiratory diseases such as COPD and heart failure (HF) are identified as at risk for development of oropharyngeal dysphagia. Additionally, patients who experience prolonged endotracheal intubation have an increased risk of developing dysphagia. (Malandraki et al., 2016) This is often seen in patients hospitalized for COVID-19.
Several studies have linked longer duration of mechanical ventilation, repeat intubation, and age to the development of dysphagia. Although many patients experience dysphagia only during hospitalization, it is not uncommon for postextubation dysphagia to persist in those experiencing a critical illness. (Coyle, 2014)
Dysphagia characteristics in patients with disrupted cardiopulmonary and/or airway function: (Martin-Harris, 2008)
- Discoordination of the respiration-swallow cycle
- Decreased movement of the larynx and vocal cords (airway protection)
- Abnormal swallowing sensation and timing
These deficits have been linked to increased episodes of penetration and aspiration, development of pneumonia, malnutrition, and dehydration.
It is imperative for the SLP to conduct a thorough Clinical Swallow Evaluation (CSE) to identify the presence of dysphagia. The CSE is a collection of non-instrumental measures which may include:
- Comprehensive review of medical history
- Medication review
- Patient interview
- Brief cognitive assessment
- Structural examination
- Cranial nerve exam
- Objective measures/questionnaires
- Trial swallows of liquids and foods
As indicated, the SLP will obtain an instrumental swallow study for further assessment that would include a video fluoroscopic swallow study (VFSS) or fiberoptic endoscopic evaluation of swallow (FEES).
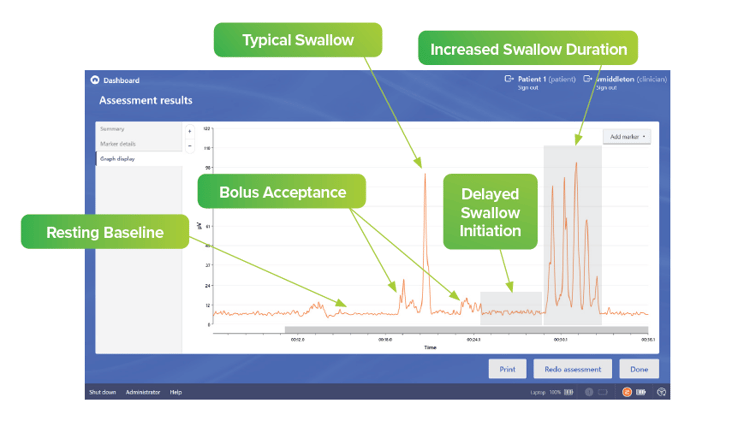
Surface electromyography (sEMG) biofeedback with Synchrony Dysphagia Solutions by ACP® for assessment during CSE provides additional insight immediately to the patient and clinician. Muscle movement is displayed in graph form to showcase the presence of excessive muscle
movement, delayed initiation of muscle movement, and disruption of swallow coordination
and duration.
Once the patient’s swallow function has been assessed, the SLP develops a treatment plan to address the specific swallowing impairment with the goal of restoring swallowing function, nutrition, hydration, and pulmonary health. sEMG can play a role throughout the treatment of patients with dysphagia.
- Adjunctive sEMG biofeedback has proven to be a beneficial adjunctive tool in swallowing therapy for cost-effective rehabilitation of people with chronic dysphagia by improving swallowing and enabling less restrictive diets. (Crary et al., 2004)
- The use of sEMG in conjunction with appropriate swallowing exercises has been shown to decrease swallow reaction times, provide superior laryngeal movement, improve swallow duration time, and assist patients in gaining greater control over tongue and throat muscle movements. (Authokorala et al., 2014)
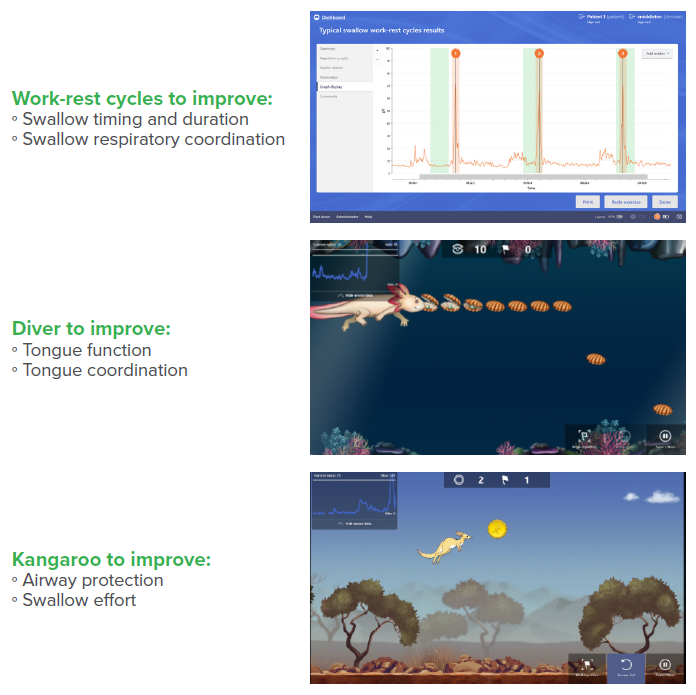
Synchrony OmnisEMG™ incorporates graphics and virtual reality visualizations during treatment to assist the patient in learning movements and exercises. For patients experiencing dysphagia due to cardiopulmonary and/or airway disorders, treatment may include the following:
For additional related resources, refer to these continuing education courses offered on ACP University. ACP is an ASHA-Approved CE Provider.
- COPD and Dysphagia
- Nutrition and Altered Diets in Dysphagia
- Considerations of Aspiration Pneumonia
- Clinical Swallow Evaluation
References:
Athukorala R, Jones R, Sella O, Huckabee M (2014). Skill training for swallowing rehabilitation in patients with Parkinson’s disease. Archives of Physical Medicine Rehabilitation, 95(7), 1374-82. http://doi.org/10.1016/j.apmr.2014.03.0011
Coyle, J.L. (2014). Dysphagia Following Prolonged Endotracheal Intubation: Is There A Rule of Thumb? Perspectives on Swallowing and Swallowing Disorders. Dysphagia, http://doi.org/10.1044/sasd23.2.800
Crary, M. A., Carnaby Mann, G. D., Groher, M. E., & Helseth, E. (2004). Functional benefits of dysphagia therapy using adjunctive sEMG biofeedback. Dysphagia, 19(3), 160-164. http://doi.org/10.1007/s00455-004-0003-8
Malandraki, G.A., Vasiliki M., Georgopoulos, V.C., Psychogios, L., & Nanas, S. (2016). Postextubation Dysphagia in Critical Patients: A First Report From the Largest Step-Down Intensive Care Unit in Greece. American Journal of Speech-Language Pathology. https://doi.org/10.1044/2015_AJSLP-14-0069
Martin-Harris, B. (2008). Clinical implications of respiratory–swallowing interactions. Current opinion in otolaryngology & head and neck surgery, 16(3), 194. http://doi.org/10.1097/MOO.0b013e3282febd4b